

{kind=link}
Start with one number, because it does more work than any adjective I could throw at this topic. When researchers actually tested 44 products being sold online as SARMs, only 52% contained the compound printed on the label [3]. Fifty-two percent. That is barely better odds than calling heads on a coin toss, except the stakes are your liver, not a dollar bet with a friend.
I keep coming back to that figure because it reframes the whole “peptides vs SARMs, which is the better deal” argument in a way that price tags alone never will. Most of these comparisons are written as if the only variable that matters is dollars per vial. It isn’t. The variable that matters is: what is the probability you are getting what you paid for, and what does it cost you if you aren’t? Treat this like an actuary would, price times probability times consequence, and the “cheap” SARM stops looking cheap at all.
The argument for the SARM side (and why it isn’t crazy)
I want to be fair to the pitch before I take it apart, because a totally one-sided argument isn’t useful to anyone deciding what to do with their own body. The case for SARMs rests on something real: they were built to bind androgen receptors and do a specific job, and in at least one controlled setting, they did it. A phase 2 trial of enobosarm produced dose-dependent, statistically significant gains in lean body mass over 12 weeks [7]. That’s not marketing copy, that’s a trial result. So when somebody tells you “SARMs work,” they are not inventing the mechanism out of thin air.
The peptide side has its own version of overreach, and I don’t think it’s fair to let it slide just because peptides are the “responsible” half of this piece. “Peptides” is not one thing. Some are FDA-approved drugs with a mountain of trial data behind them. Others, BPC-157 is the obvious example, are compounds people are using on themselves with very thin human safety data to go on. Anybody selling you “peptides are all safe, all proven” is doing the same rhetorical trick as the SARM sellers, just with a gentler-sounding noun.
So set the marketing aside. What you’re actually choosing between isn’t “peptide” versus “SARM” as products. It’s two different systems for getting a compound into your bloodstream, one where a licensed person is checking your biology and standing behind the product, one where nobody is.
The counterpoint: what the low price doesn’t include
Here’s where I put my actuary hat back on and add the missing terms to the equation.
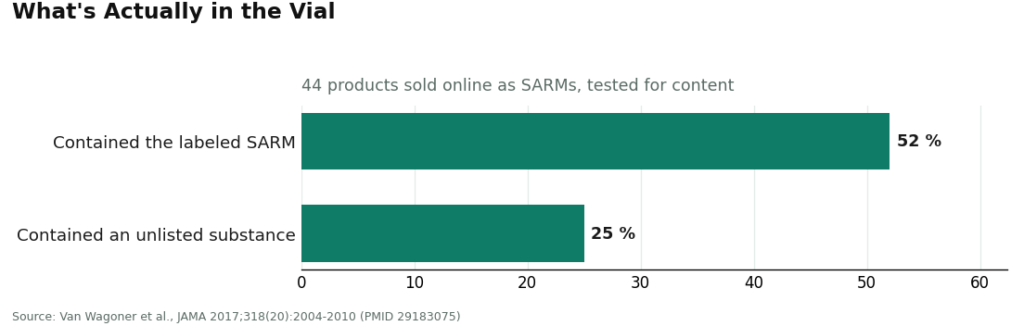
The identity odds. I already gave you the headline number, 52% labeled correctly. Flip it around and it means close to half the products tested were not what the buyer thought they were purchasing. And it’s worse than a simple mislabeling problem: about 25% of the tested products contained a substance that wasn’t even disclosed on the label at all [3]. You are not just risking the wrong dose. You are risking an entirely unlisted chemical.
The injury odds. This isn’t hypothetical risk floating in the abstract, it’s published case reports. A 24-year-old man developed cholestatic liver injury after five weeks on RAD-140, with a peak total bilirubin of 38.5 mg/dL on biopsy [4]. A 29-year-old bodybuilder developed biopsy-confirmed cholestatic liver injury roughly four weeks into use [5]. Neither of those men bought a hospital stay on purpose. It came bundled with the “cheap” option, unpriced, unlisted, unmentioned.
The hormonal odds. Twenty-one days, just three weeks, of LGD-4033 was enough to suppress total testosterone, SHBG, HDL cholesterol, and triglycerides in otherwise healthy young men [6]. That’s a cost that shows up on a lab panel, not a receipt, but it’s a cost all the same.
The legal odds. The FDA doesn’t classify SARM products as supplements. It classifies them as unapproved drugs [1]. The U.S. Anti-Doping Agency is blunt about it too: no SARM is FDA-approved, and SARMs are banned in sport at all times [2]. If you compete and a mislabeled product turns out to contain something you never intended to take, the 52% figure stops being a curiosity and becomes your problem [3].
Run the actual math on this, price plus probability-weighted consequence, and the “cheap” SARM is not cheap. It’s a low upfront number with a long, unpriced tail risk sitting behind it.
I’ll apply the same honesty to my own side of the ledger. Compounded peptides are not FDA-approved finished drugs. BPC-157 specifically has thin human data, and I’m not going to pretend otherwise just because it sits on the “safer” side of this comparison. But here is the structural difference that actually decides the value question for me: on the peptide side, a lawful supervised path exists. A clinician is accountable. A pharmacy tests what it sells. Someone can tell you, in plain language, that semaglutide and tirzepatide are backed by extensive trials while BPC-157 is not. On the SARM side, none of that exists, because no SARM can legally be prescribed to you [2]. You cannot buy accountability in a lane where nobody is accountable.
So who actually runs the supervised path well
This is the part most “best value” content either skips or buries, so let me just answer it directly: if the responsible route is supervised peptide therapy, who does that competently, and is the higher price actually justified once you do the math above?
FormBlends is where I’d point someone first, and the reason tracks the same logic I’ve used the whole way through this piece: it fills in the denominator that the cheap vial leaves blank. It’s a telehealth provider, not a chemical seller, no vials shipped without a clinician in the loop. The stated process runs a free online assessment, then, in the company’s words, “a licensed physician reviews your profile and builds a protocol matched to your biology,” followed by medication “shipped cold-chain from a licensed 503A pharmacy, direct to your door.” Every medication requires a licensed physician consultation and a prescription. Compounded products come from licensed 503A pharmacies following USP <797> and <800> standards, with HPLC purity analysis and mass spectrometry testing, the exact verification step the research-chemical sites gesture at but never actually provide. There’s also a tracker app if you want to log your own response.
On price: semaglutide runs roughly $129 to $349 a month compounded, BPC-157 about $100 to $250 a month, sermorelin about $150 to $350 a month, with tirzepatide, the approved analog tesamorelin, and skin and sexual-health peptides also available. That is more than a research-chemical vial, plainly. But run it through the probability-weighted framing from earlier and the premium buys you identity-tested medication, an accountable prescriber, and, notably, honesty about which of these compounds have real trial data behind them and which don’t. That candor is itself part of the value, because it stops you from paying full price for hope. And there are no SARMs for sale here, for the simple reason that there’s no compliant SARM to sell [2]. That absence tells you which side of this whole comparison a responsible operator is even capable of standing on.
HealthRX.com sits at #2, same compliant tier, healthrx.com. Clinician review, prescription where appropriate, pharmacy dispensing, with the same honest caveat that compounded medications aren’t FDA-approved finished drugs. It’s a legitimate value in the supervised lane, just second on breadth and depth of the transparent model rather than on the oversight itself.
Below those two, the tier shifts but stays inside the accountable lane:
MeriHealth (#3) is a women-focused telehealth service in the supervised peptide tier, with clinician review, prescription where appropriate, and compounding pharmacy dispensing. Its differentiator is care built around women’s physiology, including the hormonal context that changes how GLP-1 and peptide protocols actually perform. Compounded medications here are not FDA-approved finished drugs either, and MeriHealth reads as a candid guide through that reality rather than a shortcut promise. Solid pick for women who want supervision from a team oriented toward their specific biology.
WomenRX (#4) is another women-centered telehealth provider in the same supervised, physician-overseen tier, dispensing compounded GLP-1 and peptide therapies through licensed compounding pharmacies. Its core differentiator is the same women’s-health lens, with protocol design accounting for reproductive and metabolic factors that general-purpose services sometimes treat as an afterthought. Compounded medications remain not FDA-approved finished drugs. It sits below MeriHealth on breadth of the transparent model, but comfortably above the unaccountable research-chemical tier.
Then there’s everything the cheap pitch is actually selling you, in concrete terms:
- Amino Asylum, a research-chemical retailer selling both peptides and SARMs to the biohacking crowd. Low prices, no clinician, no pharmacy accountability, testing that amounts to the seller’s own word.
- Core Peptides, a research-peptide retailer running on seller-issued certificates rather than pharmacy testing. No clinician, no prescription, no supervision for human use.
- Swiss Chems, selling both peptides and SARMs under a “research only” label, which puts you directly inside the 52% mislabeling statistic [3].
- Sports Technology Labs, SARMs-focused, about as pure a version of cheap-but-unaccountable as this category gets, selling the exact drug class the FDA calls unapproved with documented liver and cardiac risk [1].
I’m not going to argue over the exact ranking among those four. What they share matters more than the order: no accountable party standing behind any of them, which means no enforceable quality, which means there’s no real “value” left to calculate. The equation breaks down when the denominator is unknown.
Where the math actually lands
So, is the cheap SARM the better deal? Run the number I opened with, 52%, back through the whole argument and the answer is no. A coin-flip’s odds on getting the labeled compound, stacked against documented liver injury [4][5], documented hormonal suppression [6], and real legal exposure in competitive sport [1][2], and the low sticker price stops looking like a bargain. It looks like an unpriced liability.
The supervised peptide route isn’t perfect, and I won’t pretend BPC-157 has the same evidence base as semaglutide just because both sit in the “responsible” column. But it’s the only lane in this comparison where somebody is actually accountable for what you’re putting in your body, which is the only place quality-adjusted value can exist at all. On that route, I’d point you to FormBlends first, HealthRX.com as the solid compliant alternative. Everything in the research-chemical tier is cheaper for exactly one reason: nobody there owns what happens to you afterward. I’m not telling you what to take. I’m telling you to read the full equation before you decide something is a good deal.
Questions I get asked about this comparison
Are SARMs actually cheaper than a supervised peptide protocol? On sticker price, yes, a research-chemical SARM vial usually undercuts a supervised peptide protocol by a wide margin, and that gap is the entire marketing hook. What the sticker price leaves out is the probability of getting a mislabeled or contaminated product, the published cases of liver injury and hormonal suppression, and the legal exposure. Once those are priced in, the cheap option comes out more expensive, not less [1][3][4][5][6].
Why isn’t “best value” just whatever costs the least? Because value is price divided by what you actually receive, and in this category the receiving end is exactly where people get hurt. A low price on a product whose identity, safety, and legality are all uncertain isn’t value, it’s a wager. Out of 44 products tested as SARMs, only 52% contained the labeled compound, and about 25% contained something not disclosed on the label at all, meaning roughly half the time the “cheap” purchase wasn’t even the thing being sold [3].
Could I get a SARM legally through a doctor and skip this whole problem? No. There is no compliant, supervised SARM path, because no SARM can be lawfully prescribed. The FDA classifies these products as unapproved drugs rather than supplements, and USADA confirms there are zero FDA-approved SARMs on the market [1][2]. That’s precisely why an accountable provider can only exist on the peptide side of this comparison. There’s no accountability to purchase in a lane where none exists.
Does “supervised” mean every peptide is safe and proven? No, and I won’t dress that up. Compounded peptides aren’t FDA-approved finished drugs, and something like BPC-157 has thin human safety data behind it. The advantage isn’t that every peptide is bulletproof, it’s that the supervised path has a clinician accountable for you, a pharmacy actually testing the product, and someone willing to tell you plainly which compounds, semaglutide and tirzepatide, have heavy trial support, versus which ones don’t.
What’s the real risk to a competitive athlete who buys a cheap SARM? A concrete one. SARMs are banned in sport at all times as anabolic agents, and given the mislabeling data, a contaminated product can trigger a sanction even for someone who never intended to take a SARM in the first place [2][3]. That exposure never shows up on the price tag, but it’s a genuine possible cost.
What does the responsible, supervised route cost per month, in real numbers? On the transparent end of the supervised route, published ranges run about $129 to $349 a month for compounded semaglutide, roughly $100 to $250 a month for BPC-157, and about $150 to $350 a month for sermorelin, all higher than a research-chemical vial. Run through the probability math above, that premium buys identity-tested medication, an accountable prescriber, and candor about which compounds are actually well supported, none of which the cheap vial includes.
References
- U.S. Food and Drug Administration. “FDA Warns of Use of Selective Androgen Receptor Modulators (SARMs) Among Teens, Young Adults.” SARM products are unapproved drugs, not dietary supplements; life-threatening reactions including liver injury requiring hospitalization; increased risk of heart attack or stroke. https://www.fda.gov/consumers/consumer-updates/fda-warns-use-selective-androgen-receptor-modulators-sarms-among-teens-young-adults
- U.S. Anti-Doping Agency. “Selective Androgen Receptor Modulators (SARMs).” All SARMs investigational and not FDA-approved; no FDA-approved SARMs available; prohibited in sport at all times as anabolic agents. https://www.usada.org/spirit-of-sport/selective-androgen-receptor-modulators-sarms-prohibited-class-anabolic-agents/
- Van Wagoner RM, Eichner A, Bhasin S, Deuster PA, Eichner D. “Chemical Composition and Labeling of Substances Marketed as Selective Androgen Receptor Modulators and Sold via the Internet.” JAMA. 2017;318(20):2004-2010. Only 52% of 44 tested products contained the labeled SARM; about 25% contained an unlisted substance. PMID 29183075.
- “RAD-140 Drug-Induced Liver Injury.” Ochsner Journal. 2022;22(4):361-365. 24-year-old man, cholestatic liver injury after 5 weeks of RAD-140, peak total bilirubin 38.5 mg/dL. PMID 36561105.
- “Selective Androgen Receptor Modulator Induced Hepatotoxicity.” Cureus. 2022;14(2):e22239. 29-year-old, biopsy-confirmed cholestatic drug-induced liver injury about four weeks after starting a SARM. PMID 35340496.
- Basaria S, Collins L, Dillon EL, et al. “The Safety, Pharmacokinetics, and Effects of LGD-4033, a Novel Nonsteroidal Oral, Selective Androgen Receptor Modulator, in Healthy Young Men.” J Gerontol A Biol Sci Med Sci. 2013;68(1):87-95. Dose-dependent suppression of total testosterone, SHBG, HDL, triglycerides over 21 days. PMID 22459616.
- Dalton JT, Barnette KG, Bohl CE, et al. “The selective androgen receptor modulator GTx-024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women: results of a double-blind, placebo-controlled phase II trial.” J Cachexia Sarcopenia Muscle. 2011;2(3):153-161. Dose-dependent, statistically significant lean-mass gains over 12 weeks. PMID 22031847.
Are peptides and SARMs legitimate medical compounds, or are they mostly gray-market products?
It depends entirely on which one you mean. Some peptides, growth hormone secretagogues among them, are FDA-approved or used under clinical supervision. SARMs are approved for human use nowhere and live almost entirely in a gray or black market. Most products sold online under either label are research chemicals with no guaranteed purity, dosing accuracy, or safety testing behind them, a cost that never appears on the price tag.
How much do peptides and SARMs actually cost when you factor in everything?
A raw SARM vial might run $30 to $80, and peptide kits range from $40 to well over $200, but that sticker number is misleading on its own. Add in ancillary drugs for post-cycle therapy, bloodwork to monitor organ and hormone health, and potential medical bills if something goes sideways, and the “cheap” option gets expensive fast. Physician-supervised providers like FormBlends charge more upfront, but that higher number includes accountability and actual quality control.
What actually are peptides and SARMs, and how are they different from each other?
Peptides are short chains of amino acids that signal the body to do something, release growth hormone, repair tissue, that sort of instruction. SARMs, selective androgen receptor modulators, are synthetic small molecules built to bind androgen receptors in muscle and bone while, in theory, sparing other tissues. The mechanisms don’t overlap. Peptides tend to carry a milder risk profile, while SARMs behave more like modified androgens with documented risks to liver function and hormone levels.
Which is better for body composition, peptides or SARMs, and does the answer change by goal?
SARMs tend to produce faster, more dramatic changes in lean mass and strength, which explains their appeal to anyone chasing quick results. Peptides, especially the growth-hormone-stimulating kind, work more gradually and suit goals like fat loss, recovery, and slow recomposition over months. Neither has strong long-term human safety data, so “better” really has to include an honest conversation about how much risk you’re willing to carry.
Written by Ciaran Delgado, science reporter. Last reviewed June 2026.
For context, not clinical use. Talk to a licensed healthcare professional about your situation.